Clinical Case Challenge: Just another case of Leukocytosis?
Francisco O. Conrado
D.V.M., MSc, Diplomate ACVP (Clinical)
Assistant Professor of Clinical Pathology
A two-year-old, neutered male, Pitbull presented to Foster Hospital for Small Animals for evaluation following a one-week history of progressive lethargy, inappetence, and diarrhea. He was referred to Foster Hospital when the in-hospital hematology analyzer used by the referring veterinarian detected abnormal leukocyte morphology and was incapable of providing accurate absolute leukocyte counts. Foster Hospital performed a complete blood count (CBC) which revealed a moderate normocytic normochromic anemia (PCV 24.0 % [RI 39.0-55.0], MCV 77.1 fL [RI 64.5-77.5], and corpuscular hemoglobin concentration mean (CHCM) 32.5 g/dL [RI 31.9-34.3]), a marked thrombocytopenia (44.0 K/µL [RI 173.0-486.0]), and a severe leukocytosis (365.9 K/µL [RI 4.4-15.1]). A biochemistry panel revealed mild disproportionate hypochloremia (102.0 mEq/L [RI 106.0-116.0]), mild to moderate hypokalemia (3.1 mEq/L [RI 3.7-5.4]), and a mildly elevated anion gap (20.0 mEq/L [RI 8.0-19.0]), consistent with the reported history of diarrhea and inappetence with mild metabolic acidosis.
What is Your Diagnosis?
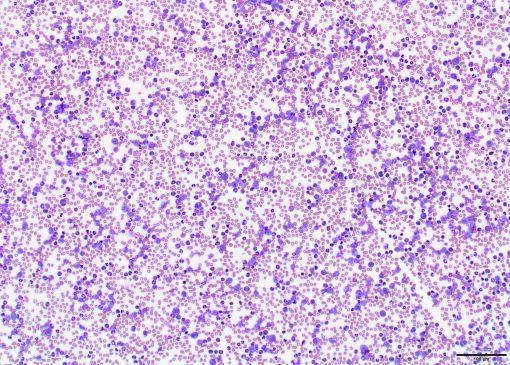
The severe leukocytosis in this patient is consistent with a leukemic process. In most of these cases, hematology analyzers have a hard time identifying the neoplastic cells and as such, evaluation of a blood smear is key for an accurate diagnosis. Most of the cells seen were atypical large cells with discrete cytoplasmic borders, a high nucleus to cytoplasm ratio, and a small to moderate amount of medium basophilic cytoplasm. The oval, reniform or irregularly-shaped nucleus of these cells measured one and a half to two and a half times the size of an erythrocyte contained coarse to clumped chromatin, and occasionally contained one to three, round or oval, discernible nucleoli that varied in size. Fewer numbers of large, non- to mildly vacuolated monocytes (91.5 K/µL [RI 0.1-1.5]) and mature, non-degenerate neutrophils (69.5 K/µL [RI 2.8-11.5]) were also noted, along with a few band neutrophils. The presence of numerous large (blast-like) cells, associated with many well-differentiated monocytes and neutrophils, is consistent with acute myelomonocytic leukemia (AML-M4). The diagnosis was confirmed with flow cytometric analysis of peripheral blood, which revealed a dramatic expansion of atypical monocytes, neutrophils with unusual light scatter properties, as well as myeloid cells that could not be identified, consistent with a myeloid neoplasm. The dog received chemotherapy, as well as supportive therapy, and exhibited mild clinical improvement, while hematologic abnormalities remained with a persistent severe leukocytosis (114.20 K/µL) at the time this article was finalized.
Acute leukemia is a hematological malignancy derived from immature hematopoietic cells. The rare proliferation of cells with myeloid and monocytic features is further classified as acute myelomonocytic leukemia (AML-M4). The definitive diagnosis of AML-M4 is typically achieved with bone marrow evaluation. Common hematologic findings include bi‐ or pancytopenia, and the overall survival time is shorter than a month, indicating a very poor prognosis. Some dogs with AML may present with peripheral lymphadenopathy (mimicking lymphoma) which illustrates the importance of a full diagnostic work-up. Evaluation of a peripheral blood smear was paramount in this case and prompted the submission of blood for flow cytometric analysis and subsequent diagnostic confirmation.
Given the drastic differences in survival times and response to chemotherapy, it is important to keep AML on the differential diagnostic list when evaluating dogs with peripheral lymphadenopathy or severe leukocytosis. Generally, the chemotherapeutic treatment of canine acute myelomonocytic leukemia is not successful, and a quick and accurate diagnosis is warranted.