Clinical Case Challenge: Just Another Neurological Symptom?
Lola, a four-year-old FS Yorkshire Terrier, presented for an episode of collapse. The owner described that Lola tried to rise from the couch, stiffened and then fell to the floor. The event lasted approximately ten seconds and it was unclear whether consciousness was retained. Lola was noted to be trembling afterward. A similar episode occurred one week earlier, and Lola has been acting a little depressed/lethargic for the past two weeks.
On presentation to Foster Hospital for Small Animals, Lola was bright, alert and responsive. Her temperature was elevated (103.8 F) and her neurologic exam was normal, except for a left head tilt and tetra-ataxia, which was worse in the hind limbs.
Q1: Based on history and examination findings, what are your primary differential diagnoses?
Given the neurologic deficits on exam, seizure seems more likely than syncope. Differential diagnoses for seizures include intra-cranial and extra-cranial causes:
- Infectious/Inflammatory – Granulomatous Meningoencephalitis (GME) vs. other
- Metabolic – hepatic encephalopathy, hypoglycemia
- Idiopathic Epilepsy
- Neoplasia – meningioma, glial tumor, choroid plexus tumor, lymphoma, vs. other
- Infarct
- Toxin – less likely without history of exposure
- Congenital malformation – hydrocephalus
Q2: What further diagnostics would you consider?
Bloodwork, urinalysis, clotting times (PT/PPT), and bile acids can all be performed to rule out extra-cranial causes of the presumed seizures. MRI +/- CSF tap are indicated to evaluate intra-cranial causes.
Diagnostics
CBC/chemistry profile: unremarkable
Urinalysis: hematuria (suspect from trauma after collapse)
PT/PTT: normal
Bile acids (fasting): normal
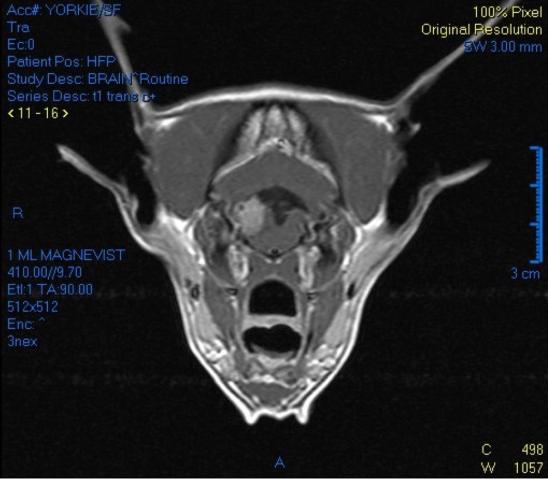
MRI (Figure 1): Right caudoventral, extra-axial mass with perilesional edema at the level of the cerebellum; suspected to arise from the lateral aperture of the 4th ventricle. The primary differential is a choroid plexus tumor (adenoma versus carcinoma); however, a meningioma cannot be completely excluded. Mild lateral ventricular and moderate 3rd and 4th ventricular distension represent secondary hydrocephalus.
Q3: What are potential treatment options?
With this type of lesion, there is worry about increased intracranial pressure (ICP) secondary to the obstruction of CSF flow. The most immediate concern is to address the elevated ICP (prednisone, ventriculoperitoneal shunt placement) with the secondary concern of addressing the tumor (radiation therapy as it is a non-surgical location).
Treatment
Lola was started on prednisone to help with the increased ICP, as well as to treat peritumoral edema. She returned the following week for ventriculoperitoneal shunt placement. Postoperatively a CT scan was performed to verify proper shunt placement and to plan radiation therapy.
Choroid plexus tumors account for 10 percent of all primary intracranial tumors in dogs. They occur most commonly in middle-aged dogs (median six-years) with a possible overrepresentation in Golden Retrievers. These tumors arise from the choroid plexus epithelium within the ventricles and consistent with grade 1 (benign papilloma), grade 2 (atypical papilloma), and grade 3 (carcinoma) tumors. Papillomas may spread locally within the ventricular system while distance metastasis to the subarachnoid space or within the ventricular system occurs in up to 50 percent of carcinomas. Metastasis outside of the CNS has not been reported. Ventriculomegaly is reported in 75 percent of cases. Distinguishing tumor grade ultimately requires histopathology, however, the presence of multiple masses on imaging and/or increased protein concentration on CSF analysis is suggestive of a carcinoma (grade 3).
Reported outcomes for choroid plexus tumors treated with radiation therapy are limited; however, in the absence of surgical options, definitive-intent radiation therapy is believed to allow for the best control over future tumor growth. A conventional definitive plan typically involves 2.5 Gy per fraction (Monday-Friday) for 20 treatments for a total dose of 50 Gy. Short-term side effects (inflammation to other tissues in the field, including the skin, oral cavity/throat, inner ears or brain) are typically quite minimal with brain irradiation. Around 3-6 months after radiation, approximately 20-30 percent of patients will experience a transient demyelination of neurons within the radiation field, which may also lead to neurologic deficits but is typically steroid-responsive. There is also a low risk (less than 5 percent) of long term effects (infarcts, necrosis, secondary tumors) within several months to years after treatment.
Newer radiation therapy options may also be considered; stereotactic radiosurgery (SRS) and stereotactic radiation therapy (SRT). These deliver either a single (SRS) or few (SRT) high dose fractions of radiation to a defined target in a highly conformal manner with the goal of achieving tumor control with strict geographic sparking of surrounding normal brain tissue in the hope of reducing the number of patient visits and toxicity. Again, literature is limited on outcome with such techniques for choroid plexus tumors but survival as long as 34.5 months have been reported with SRS.
Outcome
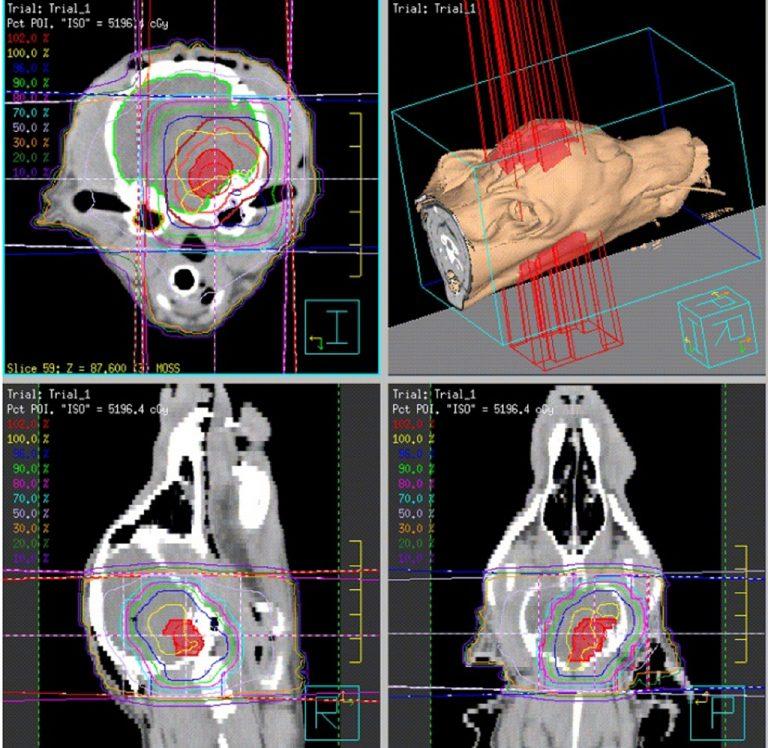
In the case presented herein, conventional definitive radiation therapy (20 fractions) was performed approximately three weeks after shunt placement (Figure 2). Lola was neurologically normal by two months post radiation and remained so until 27 months later. At that time, Lola’s owners reported recurrent tremors, possible vision loss, and an unsteady gait. Repeat MRI revealed a stable extra-axial 4th ventricular mass but progression of the peritumoral edema as well as suspect metastatic lesions within the spinal cord at C2, L3, and L5. Lola subsequently underwent stereotactic radiation to all tumor sites and was started on CCNU chemotherapy to address potential micrometastases within the CNS. She is currently doing well 34 months from her initial diagnosis.
References
- Westworth DR, Dickinson PF, Vernau W, et al. Choroid plexus tumors in 56 dogs (1985-2007). J Vet Intern Med 2008;22:1157-1165.
Department:
Foster Hospital for Small Animals